Gallbladder stones are very common, but the real problem begins when a stone does not remain limited to the gallbladder. Sometimes a stone slips into the main bile pipe, known medically as the common bile duct or CBD. This is when a simple gallstone problem can turn into jaundice, fever, infection, pancreatitis, repeated abdominal pain, vomiting, or emergency admission.
Many patients come with a familiar story: “Doctor, pain comes and goes.” “Sometimes eyes become yellow.” “Urine becomes dark.” “There was severe pain after food.” “I was told there is stone in the gallbladder and also in the pipe.” In such cases, the treatment plan must be more careful than routine gallbladder surgery.
At Arogya Hospital, Ludhiana, we commonly educate patients that gallbladder stone disease should not be judged only by pain. The surgeon must also check whether the stone has entered the bile duct. If the CBD stone is missed or treatment is delayed, the patient may suffer repeated jaundice, cholangitis, pancreatitis, or recurrent hospital visits.
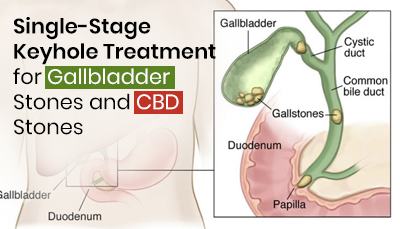
The gallbladder stores bile, which helps digest food. Bile flows from the liver into the intestine through a pipe-like channel. This channel is called the common bile duct, or CBD. When a gallstone travels from the gallbladder into this pipe, it may block the flow of bile.
A CBD stone may cause yellow eyes, dark urine, itching, fever with chills, upper abdominal pain, vomiting, abnormal liver function tests, or swelling of the bile duct on ultrasound. Sometimes the symptoms are dramatic, and sometimes the signs are subtle. This is why proper evaluation is important.
Routine laparoscopic gallbladder removal is a standard keyhole surgery for symptomatic gallstones. But when the stone is also present in the CBD, only removing the gallbladder may leave the patient’s main bile pipe blocked. Such patients need a planned strategy to clear the bile duct also.
Traditionally, many patients were treated in two steps. First, ERCP was performed to remove the CBD stone through endoscopy. Later, laparoscopic cholecystectomy was done to remove the gallbladder. This approach is still very useful in many cases, especially when urgent bile drainage is needed, when there is severe infection, or when the patient is not fit for immediate surgery.
However, in suitable patients, a modern alternative is single-stage laparoscopic treatment: laparoscopic cholecystectomy along with laparoscopic CBD exploration.
Single-stage treatment means that the gallbladder and the CBD stone are managed in the same sitting, under the same anesthesia, during the same admission, wherever medically suitable.
In this procedure, the surgeon removes the gallbladder through keyhole surgery and also explores the common bile duct to remove stones from the bile pipe. This is called laparoscopic common bile duct exploration, or LCBDE.
The surgeon uses a camera, fine laparoscopic instruments, and sometimes a special small telescope called a choledochoscope to see inside the bile duct. Depending on the case, the CBD stone may be removed through the cystic duct route or through a controlled opening in the bile duct. The exact method depends on the size of the stone, number of stones, duct diameter, anatomy, infection, and surgical judgment.
The biggest advantage of single-stage laparoscopic CBD exploration is that it aims to treat the source and the blockage together. The gallbladder, which is the source of stones, is removed, and the bile duct stone is cleared in the same planned procedure.
For selected patients, this may reduce the need for two separate procedures, two separate admissions, repeated anesthesia exposure, waiting time between ERCP and surgery, and anxiety for the family. It can also be useful when the surgeon wants to preserve the natural function of the bile duct opening as much as possible.
This does not mean ERCP is wrong. ERCP is a very valuable and life-saving procedure in many situations. But the latest thinking is not “ERCP for everyone” or “surgery for everyone”. The best approach is individualized treatment. The right patient should receive the right procedure at the right time.
Today, the evaluation of gallbladder stones and CBD stones is much more refined. Ultrasound is usually the first test. Liver function tests can suggest obstruction. MRCP, a special MRI scan of the bile duct, can map the bile passage and identify stones without putting an instrument inside the duct. In selected cases, endoscopic ultrasound may also help.
The goal is to avoid unnecessary diagnostic procedures and plan treatment properly. If the stone is confirmed or strongly suspected, the surgeon and patient can discuss whether ERCP, single-stage laparoscopic CBD exploration, or another plan is best.
Management of bile duct stones has advanced significantly. The latest tools and techniques include better imaging, intraoperative cholangiography, laparoscopic ultrasound, fluorescence guidance in selected centers, choledochoscope-assisted stone removal, advanced ERCP techniques, balloon dilation for difficult stones, mechanical lithotripsy, laser lithotripsy, and cholangioscopy-guided stone treatment.
These advances have one purpose: to make treatment safer, more precise, and less traumatic for the patient.
But technology alone is not the answer. The most important decision is choosing the correct treatment pathway. A small stone in a fit patient, a large impacted stone, a patient with jaundice, an elderly patient with infection, and a patient with pancreatitis may all need different strategies.
A patient with gallstones should seek proper surgical evaluation if there is repeated upper abdominal pain, pain after fatty meals, vomiting, fever with chills, yellow eyes, dark urine, pale stools, itching, pain going to the back, history of pancreatitis, or ultrasound showing a dilated bile duct.
These signs may indicate that the stone disease has gone beyond the gallbladder.
Repeated gallstone attacks are not just painful; they can become dangerous. A stone may block the bile duct and cause jaundice. Infection in the bile duct can become serious. A stone near the lower end of the bile pipe can trigger pancreatitis, which can sometimes be severe.
Many patients delay surgery because the pain settles after injections or medicines. But pain relief does not always mean the disease has disappeared. It may only mean that the attack has temporarily settled. The stone remains, and the next attack may be worse.
If you have gallbladder stones and your reports mention CBD stone, bile duct stone, dilated CBD, raised bilirubin, abnormal liver function tests, or obstructive jaundice, do not treat it as a simple digestion problem. You need a proper surgical and biliary evaluation.
For suitable patients, single-stage keyhole treatment with laparoscopic cholecystectomy and laparoscopic CBD exploration can be an excellent modern option. It allows the surgeon to remove the gallbladder and clear the bile duct in one planned procedure, depending on the patient’s condition and the available expertise.
The aim is not just to remove a stone. The aim is to prevent recurrence, avoid complications, reduce repeated hospital visits, and help the patient return to normal life safely.
At Arogya Hospital, near Baba Balak Nath Mandir, Jassian Road, Ludhiana, patients with gallbladder stones and CBD stones are evaluated with a practical, patient-specific approach. Some patients are best treated with ERCP first, some with single-stage laparoscopic CBD exploration, and some with staged treatment depending on jaundice, infection, pancreatitis, age, medical condition, and stone anatomy.
The best treatment is the one that clears the problem safely, at the right time, with minimum unnecessary delay.
Dr. Ashish Kumar Ohri
Consultant Surgeon
Arogya Hospital, near Baba Balak Nath Mandir, Jassian Road, Ludhiana
Patient safety note: This article is for public education. Final treatment decisions should be made after examination, blood tests, imaging reports, anesthesia fitness, and consultation with the treating surgeon.




